


1Clinical Microbiology and Infectious Disease Unit, Hospital Universitario Vinalopó, Elche, 2Department of Clinical Medicine, MiBioPath Research Group, Universidad Católica San Antonio de Murcia (UCAM), Murcia, 3Department of Dermatology, Centro Dermatológico Estético de Alicante, Alicante, 4Applied Statistical Methods in Medical Research Group, Universidad Católica San Antonio de Murcia (UCAM), Murcia, Spain, 5Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK, 6ADM Lifesequencing S.L., Paterna, 7ADM Biopolis, Paterna, Valencia, 8Health Coach S.L., Alcoy, Alicante, and 9Department of Pharmacy, Universidad Miguel Hernández de Elche, Elche, Spain
The aim of this 12-week randomized, double-blind, placebo-controlled trial was to determine the efficacy and safety of a probiotic mixture in the reduction of psoriasis severity. Ninety 18–70-year-old adults with plaque psoriasis were randomized into probiotic and placebo groups. At 12-week follow-up, 66.7% of patients in the probiotic group and 41.9% in the placebo group showed a reduction in Psoriasis Area and Severity Index of up to 75% (p < 0.05). A clinically relevant difference was observed in Physician Global Assessment index: 48.9% in the probiotic group achieved a score of 0 or 1, compared with 30.2% in the placebo group. The results of follow-up 6 months after the end of the study showed a lower risk of relapse after the intake of the probiotic mixture. Analysis of gut microbiota confirmed the efficacy of the probiotic in modulation of the microbiota composition.
Key words: psoriasis; dermatology; probiotic; microbiome; microbiota.
Accepted Aug 26, 2019; E-published Aug 27, 2019
Acta Derm Venereol
Corr: Vicente Navarro López, MiBioPath Research Group. Universidad Católica San Antonio de Murcia (UCAM). Av. de los Jerónimos, 135, ES-30107 Guadalupe, Murcia, Spain. E-mail: vnavarro@ucam.edu, vicente.navarro@bioithas.com
This clinical trial evaluated the effect of a probiotic mixture as coadjutant treatment together with topical steroids in 90 patients with plaque psoriasis. The results showed a larger reduction in the score of severity indexes in the probiotic group compared with the placebo group. Gut microbiota analysis demonstrated the efficacy of the probiotic in modulation of the composition of the microbiota. After the end of the probiotic or placebo intake, patients were followed-up for 6 months. The results showed a lower risk of relapse in patients in the probiotic group.
Psoriasis is traditionally defined as an immune-mediated, inflammatory dermatological disease charac-terized by a chronic-relapsing course and associated with multifactorial inheritance. Until recently psoriasis was considered to be a dermatological disease only, but is currently defined as a systemic one because of the involvement of multiple organs with important impact on social life and relationships (1). Social, psychological and economic impacts are comparable to other chronic diseases, such as chronic bronchitis, diabetes mellitus or depression (2). The disease affects 0.09–11.4% of the population worldwide, with variability between different countries (2).
The pathogenesis of psoriasis can be explained by dysregulation of immunological cell function, as well as keratinocyte proliferation/differentiation. Recently, the immunological pathomechanism has been substantially clarified (3). The elevation of inflammatory markers, such as tumour necrosis factor (TNF)-α, interleukin (IL)-12, IL-23 and IL-17, is characteristic in peripheral blood of patients with psoriasis (4). Treatment has been based for years on the use of topical or systemic immunosuppressants, such as systemic corticosteroids, methotrexate or cyclosporine, or phototherapy (narrow-band ultraviolet B (UVB) phototherapy, broad-band UVB or psoralen-UVA photochemotherapy) (5). In recent years, there has been marked progress in treatment of the disease due to development of drugs such as anti-TNF-α, and anti-interleukin (IL)-23 and anti-IL-17 monoclonal antibodies (6, 7). These drugs are generally more effective than topical or systemic immunosuppressants; however, there is a high economic cost and, rarely, they may cause severe side-effects, such as emergence of latent infectious diseases, such as tuberculosis or hepatitis B, which required complex treatment (7, 8). In addition, after some time, in a few cases antibodies are produced against these drugs, decreasing their effectiveness (9).
Recent findings demonstrate the presence of bacterial DNA (bactDNA) in peripheral blood samples from patients with psoriasis, accompanied by elevation in blood values of inflammatory mediators involved in psoriasis pathogenesis, such as TNF-α, interferon (IFN)-γ, IL-1β, IL-6 and IL-12, with no concurrent infectious process (10). This phenomenon is known as bacterial translocation from the intestinal lumen and is related to the integrity of the intestinal barrier, which has been described in other conditions, such as Crohn’s disease and hepatic cirrhosis (11, 12).
The microbiota is the set of microbial species present in a given habitat. Interaction of gut microbiota with the host has great relevance for development of an individual throughout their life. There is large variability among the gut microbiota in different individuals, as well as in the same person throughout their life. Among its functions the gut microbiota serves to maintain the integrity of the intestinal barrier, the degradation and digestion of nutrients, the production of fatty acids and vitamins, the reabsorption of bacterial metabolites and the firing of the immune system (13–16). The entire intestinal bacterial microbiota can reproduce rapidly while adhering easily to the intestinal mucosa. In contrast, there is an exogenous source of food intake that usually produces less reproductive capacity and less facility of adhesion to the intestine (16).
In recent years, in-depth studies have confirmed the association between the gut microbiota and certain disorders, such as cirrhosis (17), obesity (18), inflammatory bowel diseases (19), diabetes mellitus (20) and central neural disorders (21, 22). More recently our group has found the same association in patients with psoriasis, describing the “microbiome core” as a decrease in the genus Bacteroides and an increase in Akkermansia spp. compared with the healthy group (23). The understanding of these regulatory bacteria mechanisms is a challenge for medicine and a future source of new treatments aimed at treating both digestive and systemic pathologies (24, 25).
Probiotics are microorganisms that provide health benefits when consumed in adequate amounts. Mostly, they are lactic acid bacteria and bifidobacteria, which normally inhabit the intestine and can produce func-tional compounds. In general, they protect the host from infections by immunomodulation, increasing the production of immunoglobulins or activating the action of mononuclear cells and lymphocytes (26). These bacteria can colonize the intestine transiently and survive during intestinal transit. In addition, their adhesion to the epithelium modifies the local immune response of the host (27, 28). Some of them have been tested for their positive effects in pathological conditions, such as diarrhoea, vaginitis, immunological disorders, lactose intolerance, hypercholesterolaemia or food allergy (29, 30). Among them, several publications have evaluated the effect of specific probiotic strains in Crohn’s disease, a pathology with higher incidence in psoriatic patients than in the general population. Both diseases have in common the pathophysiological phenomenon of bacterial translocation (10, 31–33).
Based on previous studies, we hypothesized that the use of a probiotic may have a beneficial role in the treatment of psoriasis (10, 34–36). To our knowledge, there are no previous clinical trials using probiotics in psoriasis, hence the results obtained here are the first clinical results on the use of these microorganisms in patients with psoriasis. The primary goal was to determine the percentage of patients with clinical response during the study. For this, Psoriasis Area and Severity Index (PASI) was evaluated, considering as a positive result a PASI reduction of at least 75% of the score obtained at the beginning of the study (PASI75).
A double-blind, placebo-controlled study with randomization by baseline variables (ratio 1:1) was performed from May 2015 to October 2016. The study received approval from the Ethics Committee for Clinical Research of the Hospital General Universitario de Alicante, accredited by the Spanish Medicines Agency, and was registered in the American Registry of Clinical Trials (ClinicalTrial.gov identifier: NCT02576197).
Study population
Patients attending the dermatological outpatient clinic were asked to participate in the study if they met all of the inclusion criteria: age between 18 and 70 years, diagnosis of plaque psoriasis at least one year prior to the study, mild or moderate severity (PASI>6) and informed consent signed. In women of childbearing age, a previous negative pregnancy test was carried out and the use of barrier measures was required in their sexual relations during study participation. Patients were ineligible if they had had exposure to systemic corticosteroids, methotrexate, cyclosporine, or biologic drugs in the previous 3 months, antibiotics in the previous 2 weeks, signs of bacterial infection, the diagnosis of liver disease with Child-Pugh C index, chronic renal insufficiency with creatinine clearance < 50 ml/min or serum creatinine > 1.5 mg/dl, chronic endocrine, respiratory, neurological or moderate to severe cardiovascular disease, as well as concomitant skin disease prior to the start of the study. Criteria for withdrawal were serious adverse events at the discretion of the investigator, violation of the inclusion criteria, treatment deviation understood as 3 consecutive days without taking the medication under study and requirement of medication for another concomitant pathology not allowed in the study.
Participants, recruitment and randomization
From May 2015 to October 2016, 90 patients were recruited and evaluated by 3 dermatologists. Patients were assigned to one of the two trial arms (probiotics or control) following a computerized randomization list previously prepared by a blinded statistician for the treatment administered and for the results during all data analysis. Randomization was performed according to the baseline variables: sex, age and age of onset of psoriasis.
Procedure
All patients received treatment during the 12-week study period with topical corticosteroid betamethasone in combination with calcipotriol, according to the guidelines for the management of psoriasis (37). After being randomized, participants in the probiotic group received daily a size 0 hard gelatin capsule containing a mixture of 3 probiotic strains in 1:1:1 ratio, freeze-dried powder with maltodextrin as a carrier and patients in the placebo group received a capsule containing only maltodextrin. The probiotic and placebo capsules were matched for size, shape, and volume of contents, and were dispensed by the pharmacy department staff. The composition of this probiotic mixture was Bifidobacterium longum CECT 7347, B. lactis CECT 8145 and Lactobacillus rhamnosus CECT 8361 with a total of 1×109 colony-forming units (CFU) per capsule, formulated on maltodextrin.
This mixture of probiotics was selected based on previous data: oxidative stress has been associated with psoriasis (38), and strain B. lactis CECT 8145 and L. rhamnosus CECT 8361 have previously shown antioxidant properties in the Caenorhabditis elegans model (39). Strain B. longum CECT 7347 has an anti-inflammatory profile (34, 40) and modulates the gut microbiota (34).
The trial protocol established that patients with PASI score greater than or equal to 6 would be prescribed betamethasone dipropionate 0.25% together with calcipotriol (Daivobet®) once a day (in the night before going to sleep), and patients with PASI below 6 would be prescribed mometasone furoate 0.1% (Elocom®).
Outcome measurements
Two clinical outcomes were evaluated to determine the percentage of patients with clinical response in each treatment group during the study. For this, PASI score and PGA index (Physician Global Assessment) were evaluated at the time of inclusion, at week 2, 6 and at the end of the 12-week follow-up period. Topical steroids prescription was adjusted according to PASI observed at each visit, as explained in the previous section. Other secondary outcomes were laboratory values and, for this purpose, peripheral blood samples were collected at baseline and after 12 weeks of treatment and analysed for inflammatory markers values of TNF-α, IFN-γ, IL-1β, IL-6, IL-12 and IL-23. Finally, a stool sample was obtained from all patients at baseline and at the end of the study. The sample was immediately frozen and stored at –80°C until processing for massive genome sequencing according to our previous published strategy (23). Microbiome profiles were classified in order to better analyse the microbiome into groups based on Arumugam et al. (41), that each of the groups is named as enterotypes 1, 2 or 3 depending on higher the presence of bacteria belonging to Bacteroides, Prevotella and Ruminococcus genera, respectively. Finally the alpha diversity Shannon index, a measure of diversity that combines species richness (the number of species) and their relative abundances were calculated.
As a measure to establish the safety of the study probiotic mixture, all side-effects that appeared during the study were recorded and the results were compared between the 2 study groups.
Post clinical trial follow-up
This information was collected out of protocol study, when intervention with the probiotic or placebo had finished. Patients were followed-up during the 6 months of the post-intervention outcome period. Every month during this period, a telephone follow-up monthly visit was scheduled, and patients were asked about the clinical situation. When a patient described a relapse during this follow-up period of 6 months, he or she was requested to attend the clinic for a face to face visit, no later than 3 days after the relapse began. In the outpatient medical centre, a dermatologist evaluated the patient and documented their PASI score to assess the relapse, defined in the clinical trial as an increase in PASI score compared with the PASI result at the end of the 12-week treatment period.
Sample size and statistics
According to the trial protocol, 45 patients per group would be needed to detect a difference in clinical improvement as evaluated by the PASI score, assuming 10% lost to follow-up, 0.05 type-I error and 80% power to detect a difference of 30% of response between groups in a 2-sided t-test.
Data were analysed as intention-to-treat and the last available value was not carried forward for missing observations. Quantitative variables were summarized as means and standard deviations (SD) or median and interquartile range (IQR) and categorical variables are summarized with proportions.
The main efficacy variable was defined as binary: “a proportional reduction in PASI of 75% or more of baseline PASI” (PASI75). Following the trial protocol, once a patient reached success in a visit their outcome of success was retained for the posterior visits. At each visit we reported the probability of success in each arm with the corresponding exact 95% confidence interval (95% CI) and we compared these probabilities between the two arms using Fisher’s exact test for comparison of 2 proportions.
Regarding the analysis of PGA, we dichotomized the PGA scale into 2 categories: clear (original PGA levels “clear” or “almost clear”) vs. non-clear (rest of original PGA levels). In each visit we estimated the proportion of clear PGA in each group with exact 95% confidence intervals (95% CI) and compared these probabilities between groups using the Fisher’s exact test.
The number of days of topical steroid usage was not recorded during the trial. However, the trial protocol established that patients with PASI<6 would only be prescribed mometasone 0.1% instead of betamethasone 0.25% and calcipotriol for patients with PASI≥6. To analyse the difference in topical steroids between groups we compared the proportion of patients with PASI<6 between the two trial arms at each visit using a Fisher’s exact test. Biochemical laboratory variables and inflammatory biomarkers were analysed as continuous variables. We used linear regression models of the difference between baseline and the 12-week value, regressed on the treatment group and adjusted by the baseline value (centred on the mean of the control group) to account for regression to the mean effect. In the case of microbiome analysis, alpha diversity was conducted using the specaccum program in the vegan package as implemented for R and data was compared among each treatment groups and with those in healthy population (based on the data from the Human Microbiome Project (HMP (http://hmpdacc.org/)) following the same strategy as previously published (23). All statistical analyses were performed using statistics R version 3.2.3.
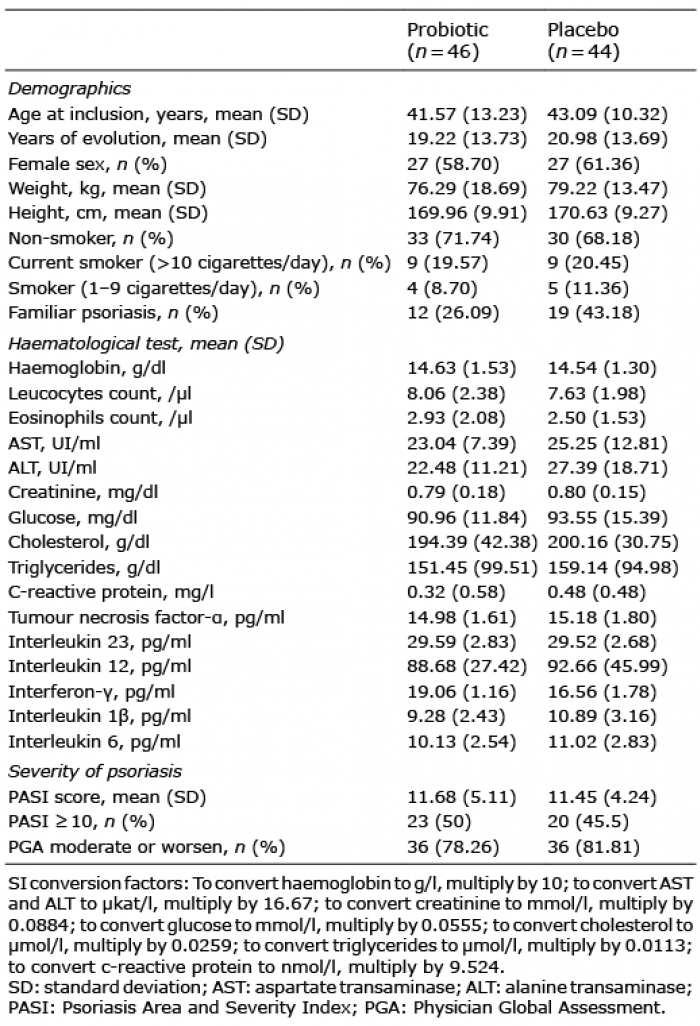
A total of 90 patients diagnosed with psoriasis were enrolled in the study and assigned to one of the two treat-ment arms. Baseline characteristics of these patients are described in Table I. CONSORT recommendations for reporting of randomized clinical trials were followed (Fig. 1). Two of 90 (2.2%) patients did not complete the study. Overall reasons for missing data were unrelated either to the treatment or to the outcome; therefore effect bias is not expected.
Table I. Baseline characteristics of study participants in both intervention groups
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) diagram.
Comparison of PASI and PGA between treatment groups
At baseline there were no noticeable differences between arms, but in the evaluation at week 12 (end of follow-up), differences arose in 30 of 45 (66.7%) patients in the probiotic group and 18 of 43 (41.9%) in the placebo group, showing a reduction in PASI up to 75% (p-value for the difference of proportions was 0.0317). Proportions and 95% CI for different weeks are shown in Fig. 2. Three of 43 (7.0%) patients in the placebo group had a severe relapse and required treatment with anti-TNF biologic drugs. The proportion of patients with PASI<6 (and therefore with no prescription of betamethasone) was greater in the intervention group than in the control group in all the follow-up visits, reaching (91%) in the probiotic group and (77%) in the control group in the last visit. However, in none of the visits the test for differences between the groups produced p-values < 0.05 (Fig. 3). PGA distributions at different visits in both groups are shown in Fig. S1. There were differences in the proportion of patients with a “clear PGA” between the two groups at week 12 visit: 22 patients (48.9%) in the probiotic group and 13 patients (30.2%) in the placebo group but the p-value for the difference of proportions was as large as 0.0853 (Fig. 4).
Fig. 2. Psoriasis Area and Severity Index (PASI)75 evolution. Point estimates with 95% exact confidence intervals of the proportion of patients with a reduction of PASI of up to 75% from baseline (PASI75) at each visit. p-values are obtained from Fisher’s exact tests comparing the 2 proportions at each time-point.
Fig. 3. Psoriasis Area and Severity Index (PASI) <6 evolution. Point estimates with 95% exact confidence intervals of the proportion of patients with PASI <6 (interrupt prescription of betamethasone) at each visit. p-values are obtained from Fisher’s exact tests comparing the 2 proportions at each time-point.
Fig. 4. Physician Global Assessment (PGA) evolution. Point estimates with 95% exact confidence intervals of the proportion of patients who reached a “clear” PGA index (as defined in the methods) at each visit. p-values are obtained from Fisher’s exact tests comparing the 2 proportions at each time-point.
Blood marker levels and microbiota composition
Baseline levels of inflammatory markers in both groups of treatment are described in Table I. No difference was observed comparing both groups of patients at the end of the intervention.
Based on the microbiome composition, the enterotype distribution of the patients at baseline was 49 (56.3%) enterotype 1, 7 (8.1%) enterotype 2, and 31 (35.6%) enterotype 3. There was no difference between the 2 analysed groups at the beginning of the study. Comparing the percentage of patients that did not change the enterotype at the end of the study in the probiotic and placebo groups, no statistically significant differences were found in any of the enterotypes (enterotype 1: 56.7% vs. 46.2%; enterotype 2: 0% vs. 42.3% and enterotype 3: 84.6% vs. 53.3%). Interestingly, there is a total disappearance of the genera Micromonospora and Rhodococcus and an increase in Collinsella and Lactobacillus in the probiotic group, comparing initial and final time-points (Fig. S2). In the case of placebo no trend was detected. Also, bacterial diversity was detected at the final time-point closer to the healthy population, although without significant statistical differences in both treatment groups (Fig. S3).
Post clinical trial follow-up
During the post study follow-up there were 9 relapses out of 45 patients (20%) included in the probiotic group, and 18 relapses of 43 patients assigned to the placebo group (41.9%) The p-value for the log-rank test was 0.027 (Fig. 5). Detailed information is shown in Table SI.
Adverse events
The number of side-effects due to interventional medication was low and, in all cases, patients continued in the study until the end of the 12-week follow-up intervention. No relevant unintended effects were associated with either the probiotic or the placebo intake. Furthermore, no severe side-effects were observed in either study group during the intervention and no patient was withdrawn due to side-effects of the treatment.
Fig. 5. Post clinical trial follow-up. Proportion of patients without a new relapse in the 6-month follow-up period in probiotic and placebo groups.
During recent years, several authors have reported the relationship between gut microbiome and psoriasis. To our knowledge, the clinical trial reported here explores for the first time the role of a mixture of probiotics administered to patients with psoriasis, both in the evolution of the activity of psoriasis and in the composition of the patients’ gut microbiota. Several variables, such as the use of antibiotics, immunomodulatory drugs and other concomitant allergenic diseases were controlled.
The results of this study show a beneficial effect of this probiotic blend, in reducing the severity of psoriasis when administered as coadjutant therapy together with topical corticosteroid. The mean variable PASI75 shows a higher response rate in patients in the probiotic group than in those in the placebo group (66.7% vs. 45.2%) at the end of the 12-week follow-up. Compared with the placebo group at the 12-week follow-up visit, the probiotic group also showed a higher proportion of patients classified as clear or almost clear in the PGA index and a lower need for prescription of betamethasone steroids (although the statistical tests did not reach 5% level of significance for either of these outcomes).
Concerning gut microbiota and its changes during the interventional period of the study, a disappearance of the problematic Micromonospora and Rhodococcus and an increase in the positive genera Collinsella and Lactobacillus were detected in the group receiving probiotics. Particularly noticeable are the elimination of Rhodococcus, a bacteria related to septicaemia and biofilm production (42), and the increase in Collinsella and Lactobacillus, genera associated with better gut health (43). An abundance of Th17 cells is notorious in skin and intestine. These cells are related to the pathogenesis of chronic inflammatory skin diseases, including psoriasis (44, 45). Intestinal microbiome contributes to balance Th17 cells and their counterpart regulatory T cells (46). Changes in the microbiota described in this clinical trial in the probiotic group could thus explain, at least in part, the positive effect of the probiotic mixture on the evolution of psoriasis.
A follow-up of patients for 6 months after the end of the intervention shows that patients previously treated with the probiotic mixture have a lower risk of relapse than those who previously received placebo. This better evolution, together with changes observed in the gut microbiota in patients previously receiving the probiotic blend, suggest a preventive role of probiotics (more time free of relapse), and not only a therapeutic benefit of coadjutant treatment.
No relevant unintended effects and no severe side-effects were observed in either group during the intervention, demonstrating the safety status of the probiotic mixture used in this study.
In conclusion, the results of this study indicate a possible positive effect of the probiotic mixture in reducing the severity of psoriasis when administered to patients with psoriasis together with the topical corticosteroid betamethasone and calcipotriol, according to the guidelines for the management of psoriasis.
Study limitations
This is the first clinical trial to assess the effectiveness of probiotics on the clinical evolution and microbiota composition of patients with psoriasis; no previous information is available for this probiotic or other probiotic strains. The fact that the study was performed in patients over 17 years of age, all from a single clinical centre, is another limitation. Finally, further limitations were the use of a single dose of the probiotic, the single period of treatment with short follow-up of 12 weeks, and the fact that the dose of topical corticosteroid was not recorded.
Conclusion
More studies that include patients from different areas, especially those consuming different diets, are necessary to further assess these results. Also, new clinical trials should consider the inclusion of patients younger than 18 years, the use of different doses of probiotics, different durations of probiotic administration and different strains, for comparison with the current results.
This study was supported by ADM Biopolis and Korott S.L.
Leticia Sánchez, BSN, and Encarna Espejo, BSN, Centro Dermatológico Estético de Alicante, provided support during the clinical and monitoring phase. No compensation was received for such contributions. We also thank all participants who agreed to take part in this trial.
Conflicts of interest: FC-C, DR-V, SG-M, and EC-C are employees of ADM Biopolis. JMP-O and JAP-M are employees of Health Coach S.L., which is a part of Korott S.L. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize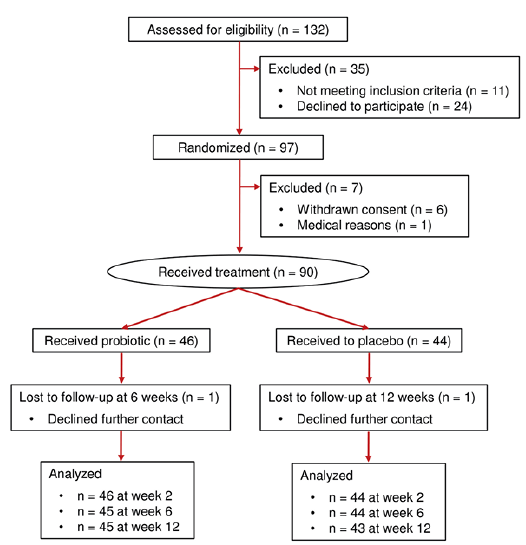 Click to show fullsize
Click to show fullsize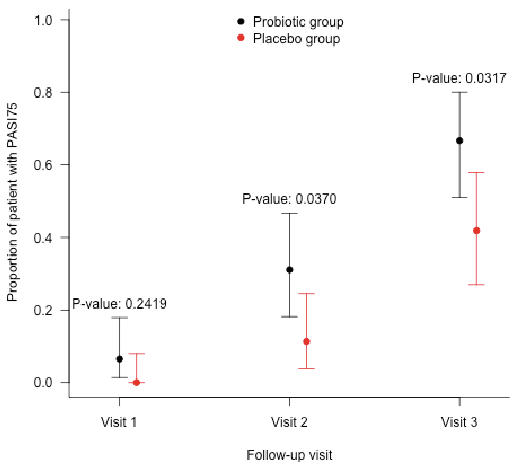 Click to show fullsize
Click to show fullsize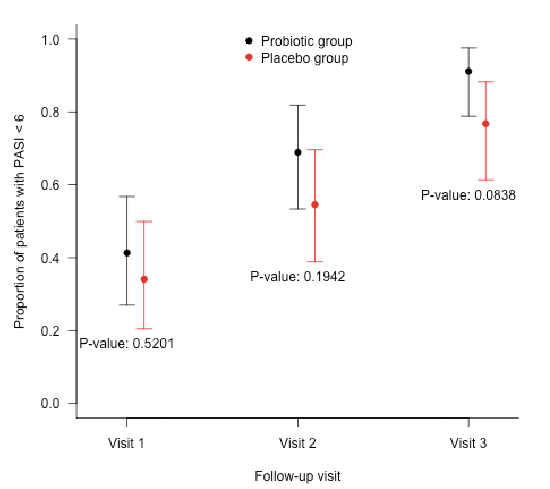 Click to show fullsize
Click to show fullsize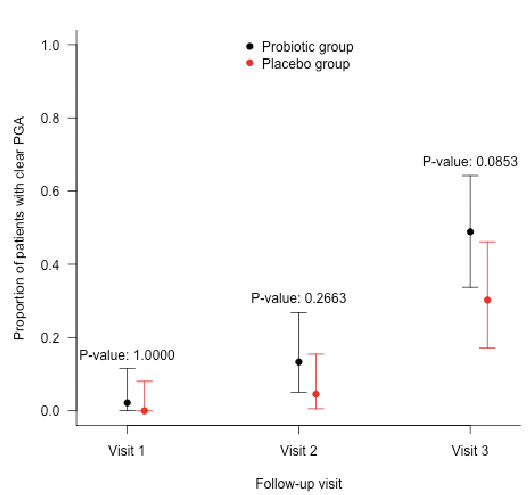 Click to show fullsize
Click to show fullsize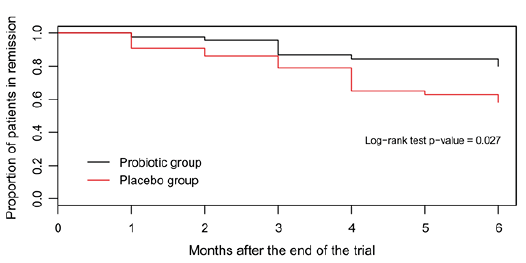 Click to show fullsize
Click to show fullsize